54
Vol. 66, No. 1 2015
Northeast Florida Medicine
Otolaryngology
middle ear contains the ossicles (malleus, incus and stapes),
which have an active role in the transfer of the sound from
the air of the ear canal into the fluids of the cochlea. The
sound transfer mechanism is accomplished by the lever
action of the ossicular chain and the size differential of
the tympanic membrane to the oval window. This results
in an extremely efficient transfer mechanism allowing a
minimal loss of sound (two decibels). The inner ear is filled
with fluid and consists of the snail shaped cochlea (two
and three quarter turns) and the balance structures. The
cochlea has a tonotopic arrangement with high frequencies
being received in the basal (outer) turn of the cochlea and
low frequency sounds being picked up in the apical (inner)
portion of the cochlea. There are approximately 16,000
hair cells within the inner ear, which have the varying roles
in the sound transduction process.
4
There are 30,000 to
40,000 afferent neurons, which relay sound information
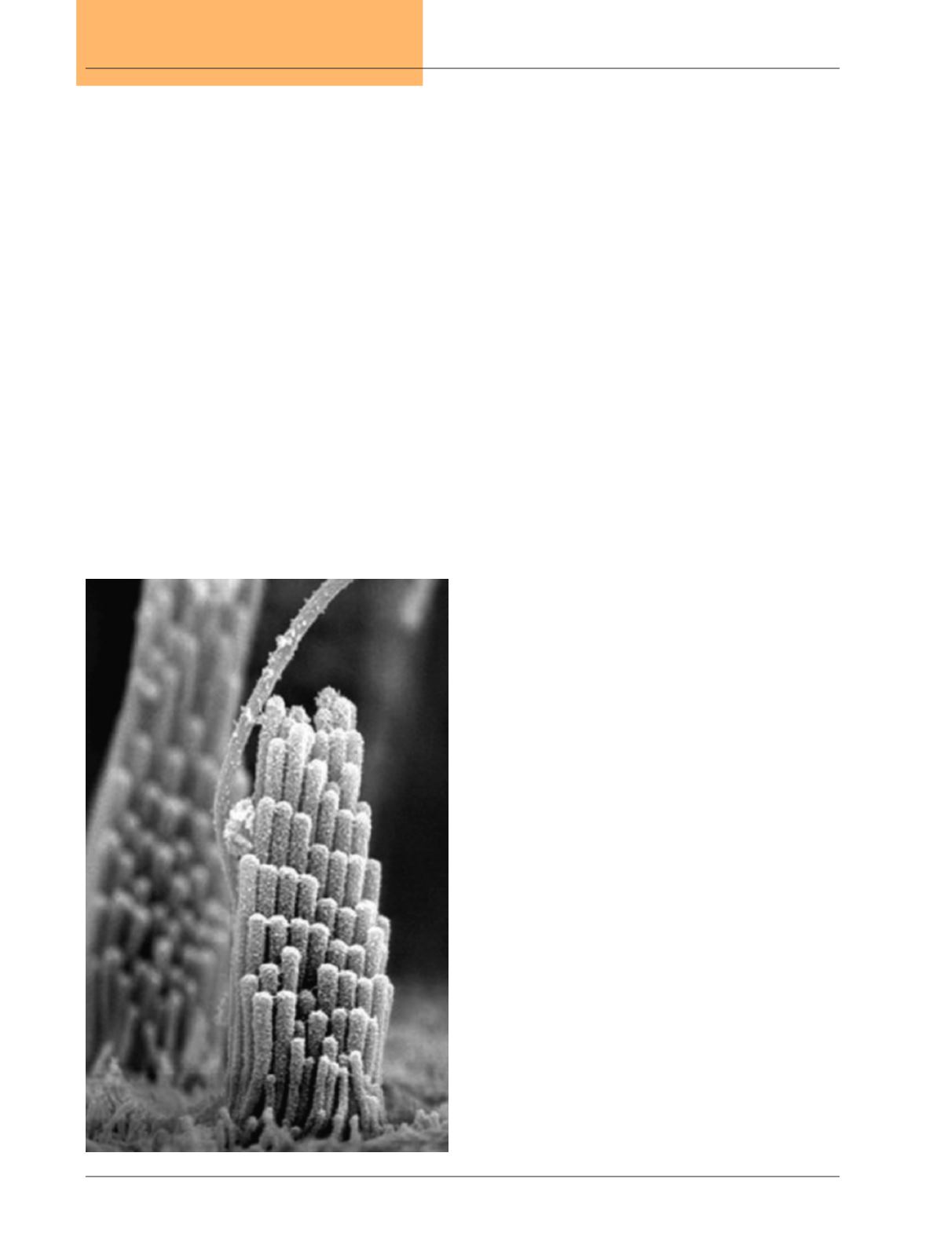
to the central nervous system. The outer hair cells act to
fine tune the region of the cochlea stimulated by a partic-
ular sound narrowing the frequency response and giving
greater clarity and acuity to the sounds being received.
(Figure 2) The inner hair cells, when deflected, open ion
channels resulting in stimulation of the hair cell. These
inner hair cell signals are transmitted through dendritic
connections to the spiral ganglia and from the spiral gan-
glia along the cochlear nerve to the brain. The brain plays
an extremely important role in sound processing with the
basic sound processing taking place in the brainstem, and
more sophisticated sound processing occurring within the
supratentorial portion of the brain, specifically within the
auditory cortex. The ears have an efficient system to detect
sound, detecting a movement of the tympanic membrane
of only a single angstrom (the size of a hydrogen molecule).
Hearing loss may be due to either a mechanical problem
resulting in a conductive hearing loss or may be due to
a problem with either the cochlea or the cochlear nerve
called a sensorineural hearing loss. At times, a conductive
component and a sensorineural component may be involved
leading to a mixed hearing loss. The simplest cause of a con-
ductive hearing loss is an accumulation of cerumen within
the ear canal. Recent clinical practice guidelines produced
by the American Academy of Otolaryngology-Head and
Neck Surgery have emphasized the importance of proper
diagnosis and treatment of cerumen impaction for affect-
ed patients.
5
Cerumen impaction should be diagnosed
when symptoms of hearing loss or occlusion are present,
or when visualization of the tympanic membrane and ear
canal are hindered by the cerumen accumulation. The
patient affected by cerumen impaction should be assessed
for modifying factors such as tympanic membrane perfo-
ration, stenosis of the external auditory canal, exostosis,
diabetes mellitus, immunocompromised status or the use
of anticoagulants. Observation of non-impacted cerumen
that is not symptomatic and does not compromise visual-
ization is acceptable. Treatment of cerumen impaction is
appropriate for affected patients and may consist of the use
of cerumenolytic eardrops, irrigation with saline or manual
disimpaction either by using a microscope or an otoscope
with appropriate instrumentation. Avoidance of Q-tips is
important as they frequently push cerumen deeper in the
ear canal and against the tympanic membrane. The Food
and Drug Administration (FDA) has advised against the
use of ear candling as a technique for removal.
6
Hearing
aids will routinely exacerbate cerumen accumulation, and
patients who use hearing aids should be assessed more
frequently for cerumen accumulation. It is important to
assess the patient after irrigation or cerumen removal to
be certain of the completeness of the removal.
Figure 2.
Scanning electron microscope imaging of the
native hair bunding from the mouse inner ear.
(Used with permission of J. R. Holt et al.,
Cell 108, 371-381 (2002))


