Northeast Florida Medicine
Vol. 66, No. 2 2015
41
CME
multi-agent vincristine and dactinomycin, and allowed
further dose-reduction of radiotherapy. In NWTS-4,
dose- and schedule-intensification of chemotherapy
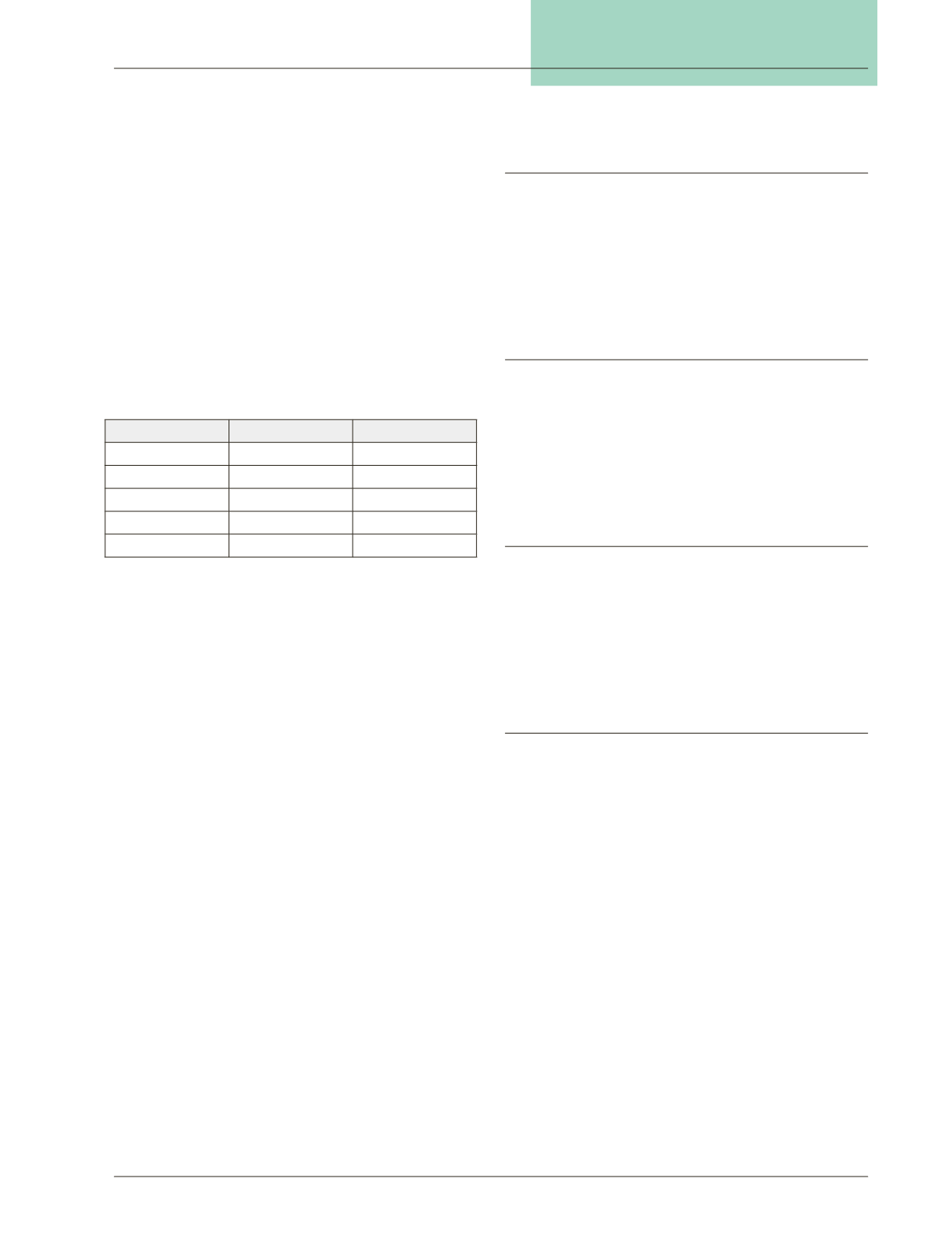
was proven beneficial. NWTS-5 utilized the optimized
schedules and doses from prior studies, considered
de-escalation of treatment for certain low risk groups,
and further evaluated risk factors for treatment failure.
Four-year outcomes from the most recent NWTS-5 study
are shown in Table 2.
Through combined efforts, NWTS and SIOP have
identified multiple prognostic factors including stage,
histology, age, and genetic polymorphisms. NWTS-1
found anaplasia to be an adverse histologic factor when
compared to favorable histologies.
8
Younger children
tend to have better outcomes than older children or
adults, especially those less than 2 years old.
9
Genetic
alterations have also been found over the last two decades
that predict for risk of recurrence. The most important
of these is loss of heterozygosity of both chromosome 1p
and 16q. The combination of both losses (LOH 1p/16q),
occurring in 5 percent of patients, is more predictive
than either alone.
10
The increased risk of recurrence is
significant enough that current trials place patients into
different treatment arms based on this finding. In stage
IV patients, another predictive factor currently being
evaluated is rapid complete response of lung metastases,
which is defined as complete resolution after six weeks
of upfront chemotherapy. This is being evaluated after a
report of NWTS-4 and 5 revealed that lung radiation did
not have a significant impact on EFS or OS for patients
with CT-detected lung-only metastases.
11
All of the above
factors must be considered when deciding the optimal
treatment regimen for any given patient.
Here we report the outcomes of patients with Wilms
tumor treated at a single institution, followed by a review
of current COG management recommendations.
Materials/Methods
A retrospective review was performed of all children
withWilms tumor treated at our institution from January
1994 through December 2012. Patients were staged by
the NWTS system and managed on- or per- COG proto-
cols. Data was compiled and analyzed in Microsoft Excel.
MedCalc was utilized to develop Kaplan-Meier plots of
progression free and overall survival for the population.
Results
64 patients were treated for Wilms tumor at our insti-
tution during the study period, with an average of 3.4
children treated per year. Median age at diagnosis was 3
years old. Stage at diagnosis was as follows: I- 17 percent,
II- 23 percent, III- 41 percent, IV- 11 percent, and V- 8
percent. Median follow up was 132 months, ranging from
20-250 months.
Management
Stage I and II patients were generally managed with
surgery and adjuvant chemotherapy. Stage III patients
were generally managed with surgery, followed by adjuvant
chemotherapy and flank/abdominal radiotherapy. Stage
IV patients were most commonly managed with surgery,
chemotherapy, and flank/lung radiotherapy. Stage V pa-
tients generally received only surgery and chemotherapy.
Recurrences
Of the 64 treated patients, there were seven patients
with recurrence (10.9 percent). There were no recurrences
in 11 patients with stage I disease.
There were 15 patients with stage II disease, of which
3 patients (20 percent) experienced recurrence. Two pa-
tients experienced a local recurrence at five months and
22 months, respectively (one of these patients actually
developed a second local recurrence three years after the
first recurrence). One patient developed a lung metastasis
17months after diagnosis. All of these stage II patients were
treated and are alive with no evidence of disease (NED).
Of 41 stage III patients, a recurrence was experienced
in three patients (7 percent). All of these recurrences were
in the lung and were experienced at four months, five
months, and seven months after diagnosis.
One out of eleven patients (9 percent) with stage IV
disease experienced a recurrence.This was a local recurrence
experienced four months after diagnosis. None of the eight
patients with stage V disease experienced a recurrence. Risk
of progression based on stage is shown in Table 3.
Stage
4-year RFS (%)
4-year OS (%)
I
92
98
II
83
92
III
85
94
IV
75
86*
V
61
80
Table 2: 4-year relapse-free survival and overall survival
rates by stage for patients treated on NWTS-5 study.
*Not found for NWTS-5 alone, but based on multiple
NWTS studies


