













 30 / 62
30 / 62

30
QRCA VIEWS
SPRING 2016
www.qrca.orgness of mental health medications has
made it tempting for healthcare insurers
to view mental health inside a medical
model (perhaps parity of coverage
between medical and mental health ser-
vices is also fueling this trend). A drug
like Celexa can reduce anxiety symptoms
and, with tweaking, can help a patient
manage anxiety for years. However, cog-
nitive behavioral therapy (CBT) and
relaxation techniques have proven to be a
more successful long-term treatment,
allowing a patient to live symptom free.
Indeed, treatment for many anxiety dis-
orders that includes therapy is more
effective than medication alone. But in
the short term, drug treatment is less
expensive for the patient and his insurer.
In addition, with insurers often cap-
ping medical evaluations at 20 minutes
for reimbursement purposes (and health
systems enforcing those 20 minutes),
psychiatrists often do not have the luxury
of time to explore everything going on
with a patient to fully understand the
scope and complexity of the patient’s ill-
nesses. Even so, psychiatrists can cause
fast relief by prescribing medication that
targets the symptoms.
In my husband’s dual diagnosis sub-
stance abuse practice, his psychiatrist
almost always ends up changing diagno-
ses and medications of the adolescents
she sees. This is a reflection not on the
skill of a patient’s previous psychiatrist
but on the substantial advantage that
comes with having the luxury of a
longer time with the adolescents and
being able to see how their psychiatric
symptoms change when their minds and
bodies are free of drug and alcohol use.
A three or four day stay at a hospital or
an initial 60-90 minute assessment just
isn’t enough time to understand what’s
going on in adolescents’ brains or their
family systems.
In Summary
Much of the conflict in mental health
research, treatment, and even in health-
care insurance comes out of battling para-
digms: brain-based or mind-based. And
the paradigms are blurring and changing
as providers sort through the treatment
implications of the neurophysiological
(i.e., hardwired) foundations of emotions,
social engagement, and self-regulation.
The opportunities for QRCs abound in a
field where an expanded number of insur-
ers are now playing and where new mind/
body treatments as well as pharmaceuticals
are battling for attention and proof of effi-
cacy. QRCs may find themselves part of
efforts to help in several ways:
• Providers (and some insurers) will
explore how to leverage technology for
web-based therapy sessions, apps that
match issues to therapies or consumers
to providers, and apps that deliver
therapies (e.g., phone apps to focus on
breathing to relax).
• Insurers will offer mental health cover-
age that is appealing and cost effective.
• The industry will need to better iden-
tify behavioral motivators so that
patients stick with treatment therapies.
• Marketing efforts will continue to
need testing of messaging and devel-
oping ad concepts.
“Perspectives on
mental health trends
run hot —explanations
vary in scope and
inflammatory tone.”
Dying from Overdoses and Other Mental Health Trends
CONT INUED
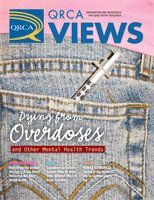
18% of americans suffer from anxiety disorders
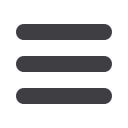
cooking heroin