18
Vol. 66, No. 3 2015
Northeast Florida Medicine
Endovascular Neurosurgery
steered to a certain degree. This allowed for a more distal
and more precise placement of the catheter in the cerebral
circulation. Physicians could accomplish temporary balloon
occlusion of selected vessels, or create permanent occlusion
of vessels feeding AVMs, or arteriovenous fistulas (AVFs).
In some cases the balloons could be placed inside cerebral
aneurysms. Serbinenko famously published a series of 304
cases of temporary balloon occlusion and 162 cases of
permanent balloon occlusion for diagnosis and treatment of
intracranial vascular lesions with excellent results in 1974.
16
This was the first report demonstrating the feasibility of
endosaccular balloon occlusion of cerebral aneurysms with
preservation of the parent artery. Later refinements included
a truly detachable microballoon with a valve mechanism.
(Figure 2) This developement was soon followed by the
calibrated-leak balloon catheter developed by Kerber in
1976.
17
This flow-directed balloon-tipped catheter had a
calibrated leak incorporated in the balloon. This allowed
for both very distal navigation and precise delivery of liquid
embolic agents through the balloon tip. It ushered in the
era of precise embolization of AVMs and AVFs with liquid
embolic agents such as Isobutyl 2-cyanoacrylate or IBCA
(better known as Super Glue).
The Emergence of a Subspecialty
Despite the obvious advantages of balloon-tipped
microcatheters, the technology was not yet to the point
where endovascular therapy could claim to be a viable
alternative to surgery for most conditions. Balloon-tipped
microcatheters generally followed the vessel with the
most flow. This limited their steerability in distal vessels.
On occasion, one would be required to place a second
microcatheter to “block” the higher flow vessel and force
the catheter into the desired channel. Detachable balloons
were not the answer for cerebral aneurysms.The balloons did
not conform to the aneurysm shape. They were associated
with higher rates of procedural rupture, lower rates of
aneurysm occlusion, and higher rates of recanalization.
18
Before endovascular therapy could challenge surgery as
preferred therapy two things would be required: A better
catheter and a better occlusion device.
The better catheter came about with the development of
the Tracker “over the wire” microcatheter in the 1980s. A
creation of Engleson, the Tracker catheter had a variable
stiffness shaft design, providing more support proximally,
and a hydrophilic coating allowing for improved trackability.
It had a steam shapable deflecting tip, and it could be
maneuvered over a steerable guidewire.
19
The catheter
could be much more easily navigated around tight curves
and across intracranial arterial bifurcations. This allowed
for a much more controlled direct catheterization of distal
vessels and cerebral aneurysms.
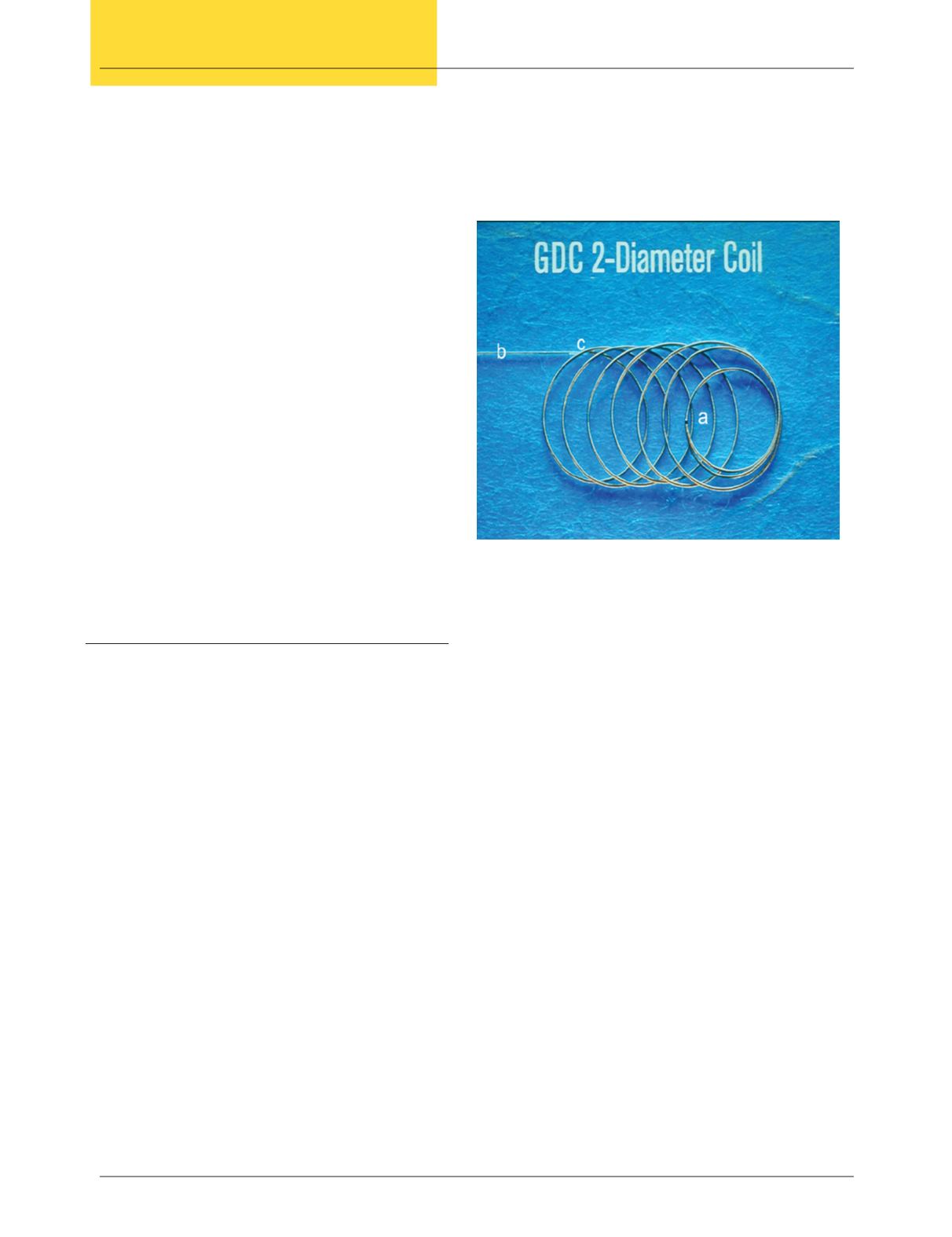
The better occlusive device came in the formof Guglielmi
Detachable Microcoils (GDC) (Figure 3.) The concept
for the coils came while searching to refine the long-
ago explored concepts of placing a foreign body in an
aneurysm, using a magnet to attract iron microspheres in
an aneurysm, and applying current to promote coagulation
in an aneurysm.
20
While applying current to a magnet
placed within an aneurysm model, the researchers eroded
the stainless steel wire holding the magnet, detaching
the magnet by electrolysis. A precise delivery system was
developed where platinum GDC microcoils attached to a
stainless steel delivery wire could be placed and replaced
until they are in an ideal position. Current could then be
applied, electrolytically detaching the coil in position and
providing some impetus for electrothrombosis.The process
could be easily repeated to fill the aneurysmwith detachable
coils.
20
The improved catheter and new coil systemdelivered
an effective embolic device to distal locations easily, and
provided precise placement in the aneurysm.This alternative
to surgical therapy for cerebral aneurysms can provide equal
or better morbidity and mortality for aneurysm patients.
The first GDC coil was placed in a patientMarch 6, 1990.
21
The rise of what is now called “neuroendovascular surgery”
Figure 3: Platinum detachable microcoils
A. Microcoils
B. Delivery wire
C. Detach zone


