Northeast Florida Medicine
Vol. 66, No. 3 2015
23
Endovascular Neurosurgery
The first decision that must be made is whether to treat
the AVM. This is a complex decision based on multiple
factors including the patient’s age, medical history (in
special presence of hemorrhage), patients’ wishes, the
AVM grade, and the experience of the treating physician.
There are several currently practiced strategies to treat an
AVM: (1) microsurgery alone, (2) radiosurgery alone, (3)
embolization alone, (4) embolization plus microsurgery,
and (5) embolization plus radiosurgery.
AVM Treatment Modalities
Microsurgery
Surgery has a long track record in the treatment of AVMs.
The effectiveness ofmicrovascular AVMresection for prevent-
ing hemorrhage and reducing seizures in patients who present
with epilepsy has been established (Figure 1).
7,8
Although
advances in microsurgery over the past three decades have
resulted in a dramatic increase in the feasibility of AVM
resection, it is clear that certain AVMs are associated with
unacceptable surgical risks.The Spetzler-Martin grading scale
attempts to quantify this differential risk by analyzing three
AVMfactors: size, venous drainage pattern, and eloquence of
congenital, arising during approximately the third week of
gestation. At that point an arrest or aberration in vascular
development results in the formation of direct arteriolar to
venous communications without an intervening capillary
bed.
2
Occasionally, an AVM can contain a true fistulous
connection between the arterial and venous side (i.e., the
arterioles empty directly into the draining veins without an
intervening nidus).
Cerebral AVMs occur in approximately 0.15 percent of
the American population and ninety percent are supra-
tentorial.
4
AVMs are one of the most common causes of
hemorrhage in young adults. Ondra et al. found cerebral
AVMs to have a yearly hemorrhage rate of 4 percent and
a yearly combined morbidity and mortality rate of 2.7
percent.
1
Certain angiographic features, such as venous
stenoses and intranidal aneurysms, have been associated
with a more aggressive course.
5,6
AVMs can cause headaches,
seizures, and ischemia related to steal. Steal is defined as
a reduction in blood flow to areas adjacent to the AVM,
because blood flow follows the path of least resistance
through the AVM. Although all AVMs can be formidable
to treat, large and deep-seated AVMs pose special problems
and often require multimodality treatment.
4
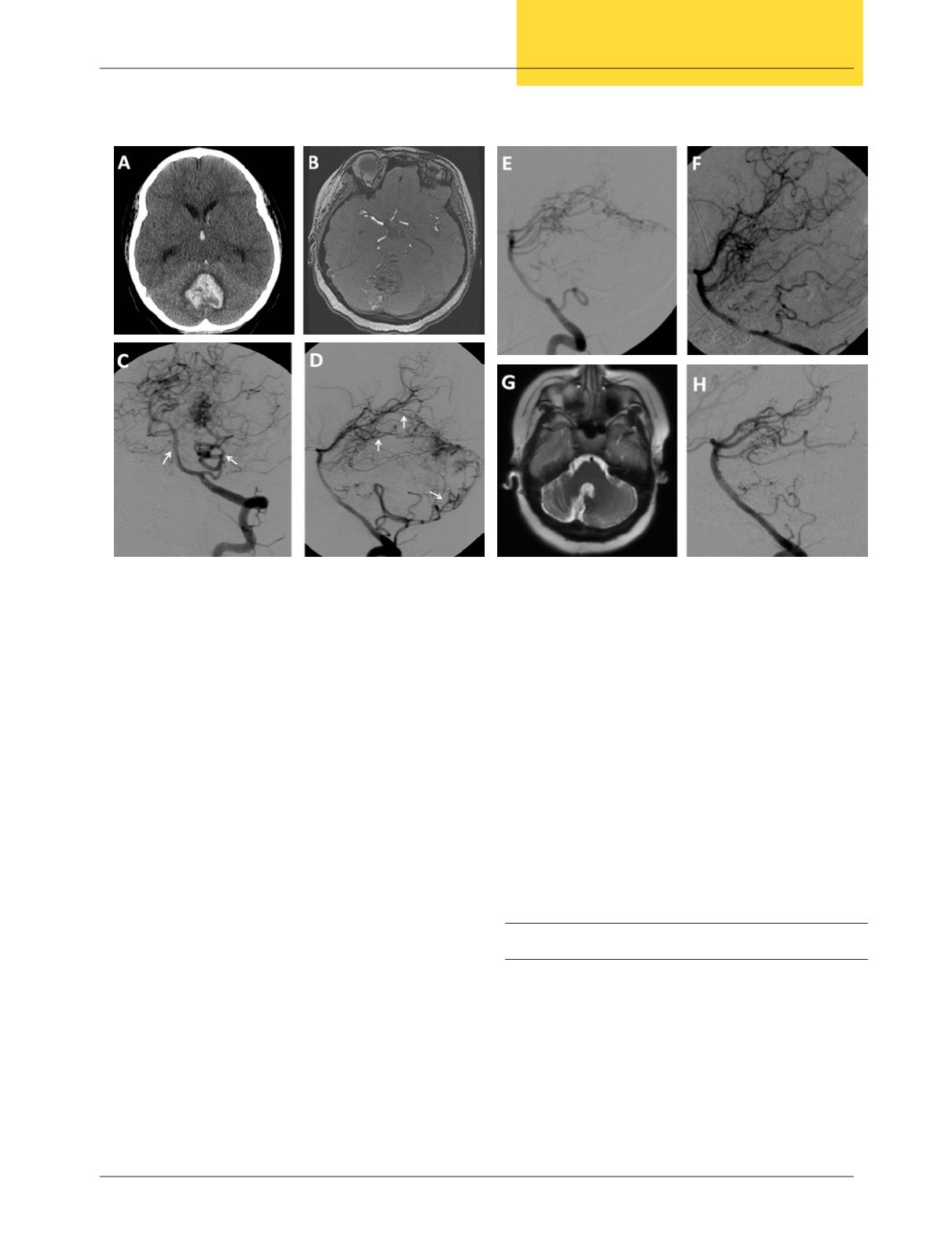
Figure 2.
An 11-year-old female was admitted with sudden headache and loss of consciousness. (A) CT scan demonstrated an
area of hemorrhage in the posterior fossa with extension into the third ventricle. (B) MRI with contrast showed a heterogeneous
lesion involving the cerebellum. (C-D) DSA in multiple views depicted the AVM and allowed us to locate the arterial feeders to
the AVM (white arrows). (E-F) Preoperative embolization of the AVM was carried out to optimize the safety and effectiveness of
surgical resection. (G-H) Follow-up images 2 years after surgery confirmed cure of the AVM.


