Northeast Florida Medicine
Vol. 66, No. 3 2015
27
Endovascular Neurosurgery
Introduction
In the past two decades the treatment of intracranial an-
eurysms has seen a paradigm shift from open neurosurgical
techniques to minimally invasive endovascular procedures.
Evidence from randomized clinical trials including the
ISAT1 (International Subarachnoid Aneurysm Trial) and
BRAT2 (Barrow Ruptured Aneurysm Trial) have provided
the impetus to support an “endovascular first” with respect
to the treatment of certain types of intracranial aneurysms.
The available endovascular devices have also quickly evolved.
This new era of endovascular treatment has achieved more
durable reconstruction of vessels and enabled treating phy-
sicians to tailor sophisticated treatment strategies for even
the most complex intracranial lesions.
Management of Intracranial Aneurysms
In general, the most important management strategy for
an intracranial aneurysm is to differentiate between ruptured
and unruptured lesions. This is due to the radically different
natural history and outcomes from treatment.
Ruptured Aneurysms
After an aneurysmal subarachnoid hemorrhage (SAH), the
primary goal of treatment is to secure the ruptured aneu-
rysm and prevent further bleeding. These lesions are almost
always treated provided that the patient is neurologically and
medically stable enough to undergo therapy. At some institu-
tions, treatment is typically carried out urgently, rather than
emergently (first 72 hours). However, recent evidence points
to the benefit of treatment within 12 hours of hemorrhage.
3
For ruptured aneurysms amenable to either open surgical or
endovascular treatment, there is evidence to support better
long-term clinical outcomes with endovascular techniques.
2
Placement of embolization coils inside the aneurysm sac
is the preferred treatment option for ruptured aneurysms,
because it obviates the need for dual antiplatelet therapy
associated with other endovascular devices and allows the
operator to preserve access to the aneurysm in the event of
future treatment. In contrast, patients with lesions anatom-
ically not amenable to coiling, or patients with expansive
hematomas are operated upon immediately to evacuate
the hematoma and secure the aneurysm. This strategy also
allows placement of the external ventricular drain (Figure 1).
After securing the aneurysm, all SAH patients are treated at
the neurointensive care unit to obtain close monitoring of
intracranial pressure, hemodynamic parameters, andmedical
complications. In addition, these patients are at an increased
risk to develop arterial vasospasmand cerebral ischemia from
breakdown of blood products into the subarachnoid space.
Timely recognition of vasospasm is paramount to prevent
severe neurological morbidity.
The Endovascular Treatment of Intracranial Aneurysms
By Leonardo B. C. Brasiliense, MD, Eric Sauvageau, MD, and Ricardo A. Hanel, MD, PhD
Abstract:
The advent of endovascular therapies for intracranial
aneurysms has completely changed the landscape for patients and
physicians. The safety and clinical results of lesions previously consid-
ered challenging and complex for microsurgical clipping has increased
significantly. Enthusiasm, increased expertise with endovascular
techniques, and collaboration between physicians and engineers
has spurred a wave of innovation that has shifted the fundamental
treatment strategies. Today, “hybrid” cerebrovascular neurosurgeons
are able to tailor the management of ruptured and unruptured
aneurysms with a large number of options ranging from microsurgical
clipping to endoluminal and intravascular devices.
Address correspondence to:
Ricardo A. Hanel, MD, PhD
800 Prudential Drive – Suite 1100
Jacksonville, FL 32207
Telephone: 904-388-6518
Fax: 904-384-1005
Email:
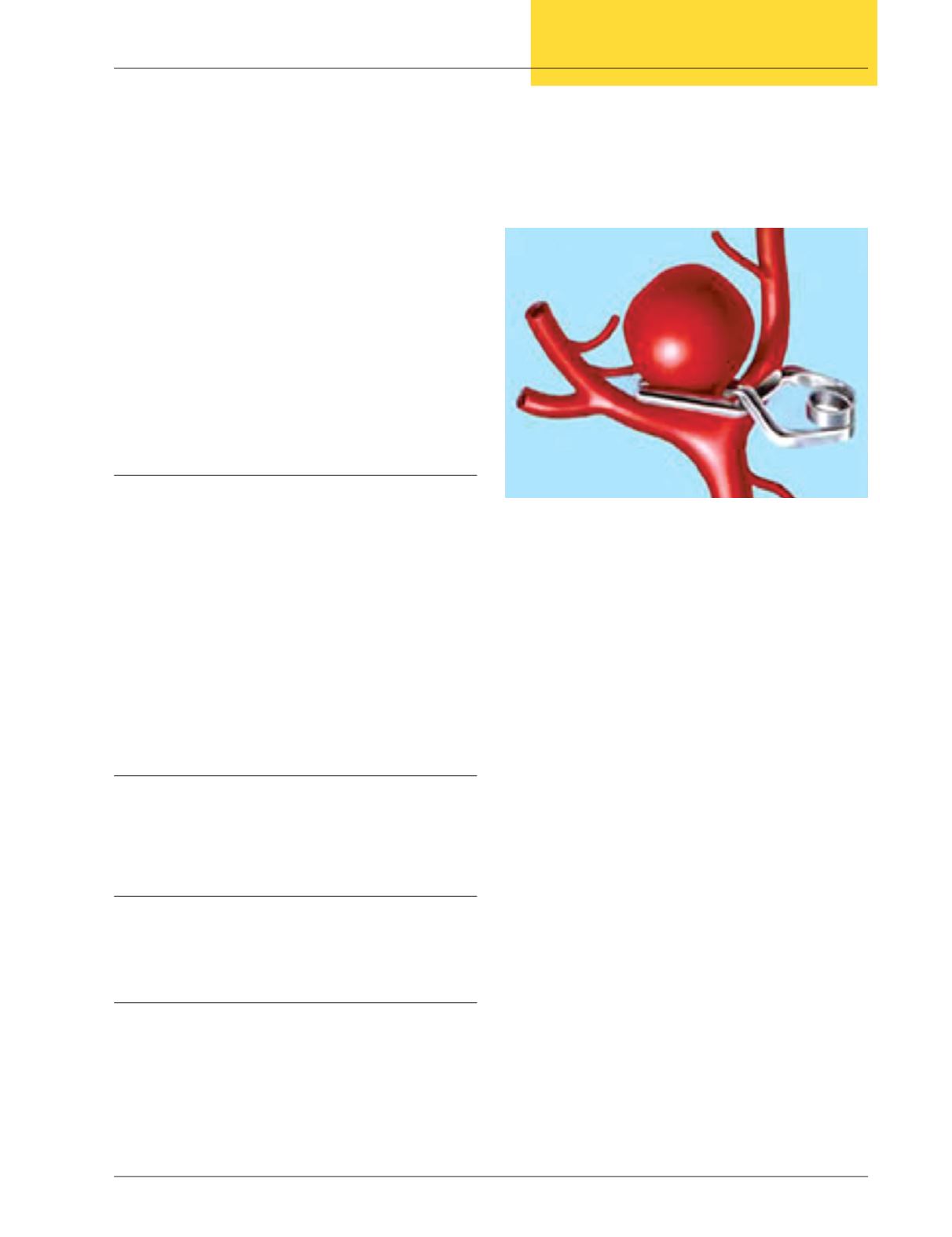
Figure 1:
After a craniotomy is performed, the
neurosurgeon dissects around the aneurysm and places a
metallic clip at the neck of the lesion to prevent a bleeding
event. This surgical technique is performed under a microscope
and represented the mainstay of aneurysm treatment before the
advent of endovascular techniques.


