Northeast Florida Medicine
Vol. 66, No. 3 2015
19
Endovascular Neurosurgery
from that time on has been meteoric. The innovations have
kept coming, and now endovascular therapy takes its place
beside surgery for the treatment of neurovascular diseases.
The other articles in this issue outline the current practices
for treatment of aneurysms, AVMs, dural fistulas, and new
therapies for acute stroke. They are high tech solutions,
built upon the shoulders of pioneers who took personal and
professional risks to push forward with innovative solutions
to tough problems.
Beyond Coils: Stents and Flow Diversion
Detachable coils allowed for the endovascular treatment
of some cerebral aneurysms. However, they had a significant
limitation with regard to aneurysm geometry. Lesions
with wide openings on the parent vessel (referred to as the
“neck” of the aneurysm) could not be treated, as the coils
could not be contained within the aneurysm. Techniques
were developed to allow for the treatment of more complex
and irregular aneurysms. These included the use of micro
balloons to temporarily occlude the aneurysm neck during
coil placement.
22
This was followed by the use of small
intravascular stents to place a scaffold across the neck to help
hold the coils in place.
24
While these additions did extend
the range of aneurysms that could be treated with detachable
coils, the technique still required entering the weakened vessel
to occlude the flow.
Recently, a new type of device has emerged, representing a
true paradigm shift in the way cerebral aneurysms are treated.
Flow diverters are a class of device placed across the aneurysm
neck to occlude aneurysms.
23,24
The devices essentially provide
for endoluminal reconstruction, as opposed to filling of the
aneurysm sac to promote thrombosis within the aneurysm.
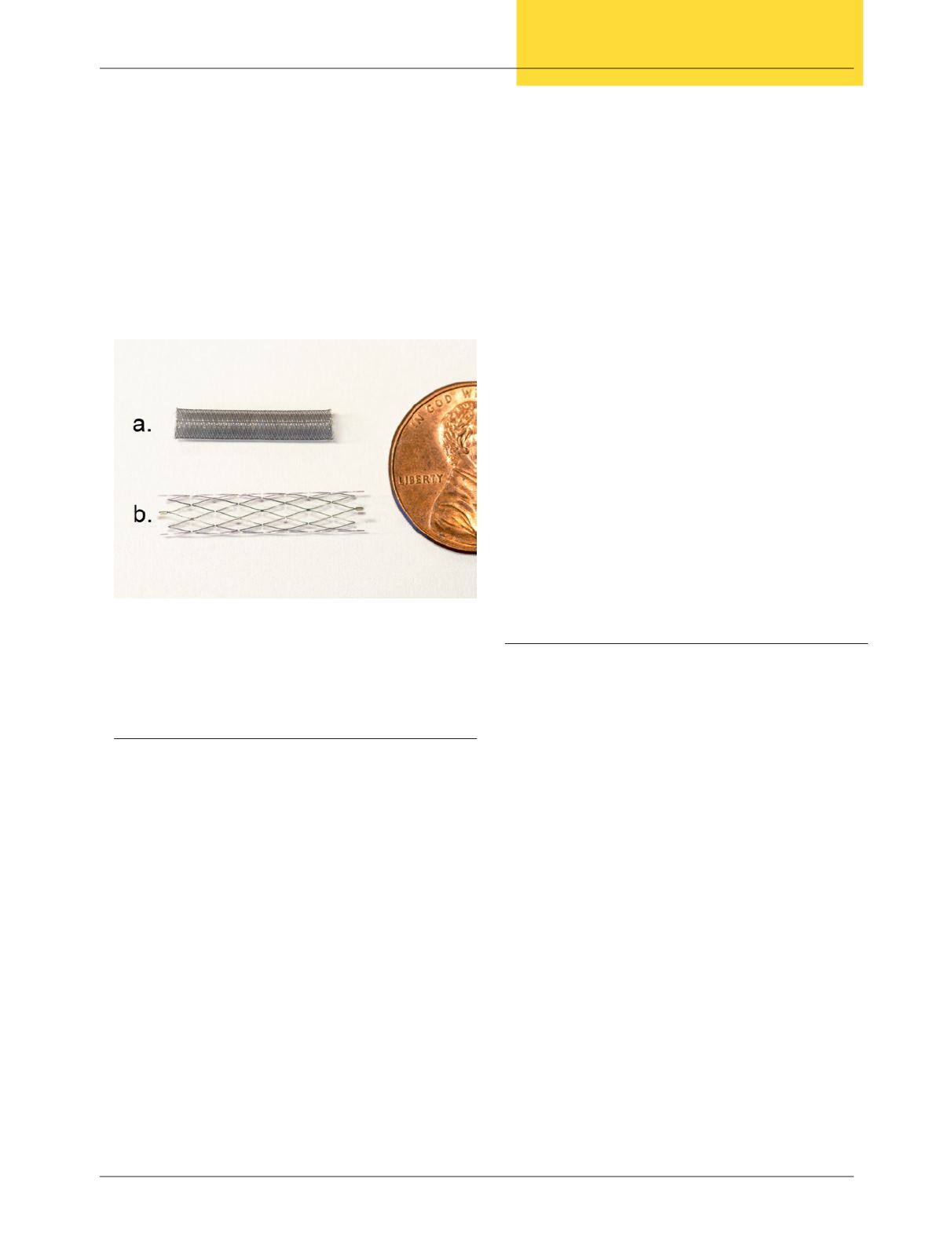
The devices look similar to traditional intravascular stents.
However, they have amuchdifferent design.Traditional stents
are designed simply to create scaffolding inside the vessel.They
have relatively large interstices (or pores), and do not provide
a significant barrier to flow. Flow diverters have much smaller
interstices (a much tighter weave so to speak) (Figure 4). This
allows for several important physiologic actions. The tighter
weave dramatically slows flow across the wall. This dramatic
decrease in flow results in stasis of blood in the aneurysm and
thrombosis, without the need for entering the sac and placing
coils. Another effect of the small pore size is that it allows for
the growth of endothelial cells across the pores. This results
in the reconstitution of the endothelial lining, providing a
true “healing” of the vessel wall.24 While still relatively early
in our experience, these devices have greatly expanded the
aneurysms that can be treated. Early results suggest a high
success rate with increased patient safety.
25,26
Conclusion
Neurosurgical endovascular therapy can trace its origins to
treatments devised centuries ago. It has taken a few hundred
years of technical innovation to allow for the practical
application of these ideas. However, it is clear that the future
of neurosurgical treatment lies in the endovascular realm, with
the promise of less invasive, safer, andmore targeted therapies.
Innovations continue, with new agents and devices emerging
to address problems such as cerebral aneurysms, arteriovenous
malformations and dural AV fistulas, stenosis of intracranial
vessels, and acute stroke. The following articles in this issue
outline the current endovascular practices for treatment of
these often complex diseases. They also cover some new and
exciting therapies for acute stroke.These arehigh techsolutions,
built upon the shoulders of pioneers who took personal and
professional risks to push forward with innovative solutions
to tough problems.
v
Figure 4: Flow Diverter and Traditional Stent
A. Flow Diverter
B. Traditional Stent


