Northeast Florida Medicine
Vol. 66, No. 3 2015
29
Endovascular Neurosurgery
in individuals with other risk factors such as polycystic
kidney disease or fibromuscular dysplasia (Table 1).
Ultimately, treatment recommendations for unruptured
aneurysms fall under three categories: (1) conservative man-
agement (including imaging surveillance), (2) microsurgical
clipping, or (3) endovascular treatment. The patient is
guided by the physician to the final decision based on the
best available information regarding all treatment options.
Aneurysm Treatment
Detachable embolization coils
The modern era of endovascular treatment for intracranial
aneurysms occurred with the FDA approval of Guglielmi de-
tachable coils (GDC) in 1995.10 The GDC system consists
of soft platinum coil soldered to a stainless steel delivery wire
(Figure 2). After the coil is navigated into the aneurysm sac, a 1
mA current is applied to the deliverywire.The current dissolves
the stainless steel delivery wire proximal to the platinum coil
and deploys the coil at the appropriate location. The process
is continued until the aneurysm is densely packed with coils
and no longer opacifies during diagnostic contrast injections
(Figure3).Thistechniqueremainsoneofthepillarsofaneurysm
management and is particularly advantageous following acute
rupture where aneurysm occlusion can be obtained faster and
less invasively (Figure 4). Complex-shaped, three-dimensional
coils were later introduced to facilitate the embolization of
more complex lesions.
Balloon Remodeling
Unfavorable anatomy, such aswide-necked aneurysms, was a
major impediment to GDC coil embolization. Prolapse of the
embolization coil into the parent artery could occur, causing
potential thromboembolism or complete vessel occlusion.
Balloon-assisted coiling was developed in the late 1990s for
the treatment of wide-neck aneurysms.
11
Briefly, a temporary
occlusionballoonmountedonamicrocatheter is navigatedand
inflated across the neck of the aneurysmwhile the embolization
coil is introduced in the lesion (Figure 5).The balloon prevents
prolapse of the coil into the parent artery. This technique is
repeated sequentially until occlusion of the aneurysm has been
achieved. However, in some instances the introduced coil
Figure 4:
Digital subtracted angiogram depicting the
anteroposterior view of a carotid terminus aneurysm before (left)
and after complete occlusion of the aneurysm with detachable
embolization coils (right).
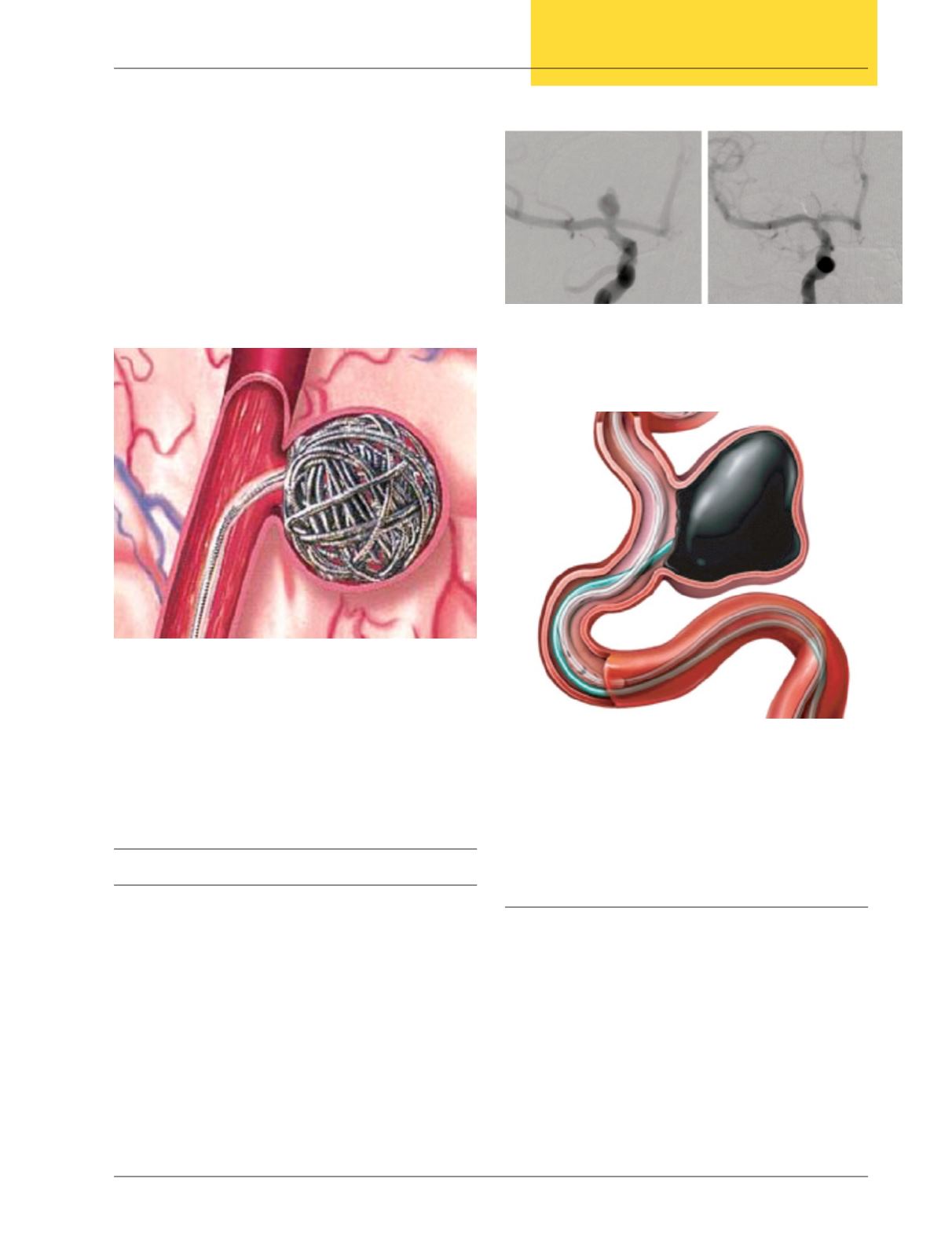
Figure 3:
Illustration demonstrating embolization coils
inside an aneurysm. After a microcatheter is inserted inside
the aneurysm sac, the embolization coils are sequentlly placed
until the aneurysm shows minimal filling at contrast injections.
Ideal aneurysms for this technique have a narrow neck to avoid
prolapse of the coils into the parent artery.
Figure 5:
Balloon-remodeling techniques advance a balloon
mounted on a microcatheter across the aneurysm neck and inflate
to provide support in aneurysms with a wide neck and prevent
complications with embolization coils or liquid embolic agents.


